After an ACL tear, most active people will benefit from ACL reconstruction.
ACL reconstruction consists of placing a graft to replace the torn ACL. But, where do we get that graft from? Well, there are several options.
First, where does it come from? Autograft vs. allograft
There are 2 techniques to obtain a graft.
- Autograft: the graft comes from the patient. They will remove one part of your tendon and use it as your new ACL.
- Allograft: it comes from a dead donor. Same thing we do with liver or heart transplants, but you get a tendon.
Is it safe to use a graft from a donor? It’s perfectly fine. Many years ago, there were concerns about getting some diseases if the donor was infected—like HIV or hepatitis. Nowadays every donor is tested before using their organs, so it’s a safe procedure
Using your own tendons for ACL reconstruction
Autograft means doctors get the graft from one of your tendons. There are several they can use, the main ones being:
- patellar tendon
- hamstring tendon
- quadriceps tendon
All of them are good choices, but there are subtle differences between them. Let’s see them:
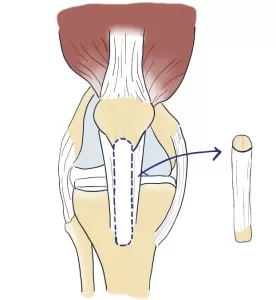
· Patellar tendon
They’ll remove one strap of your patellar tendon, which goes from the patella (or kneecap) to your shin. Also, they’ll remove a small piece of bone from each.
It works very well and we use it for high-demand athletes.
The only downsides are:
- You can have some pain behind your kneecap, especially with kneeling.
- Sometimes there may be some stiffness.
- There is some risk of a kneecap fracture.
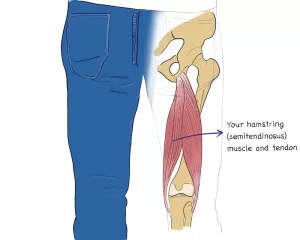
· Hamstring tendon
In this case, they harvest the graft from your hamstring tendon, which is on the back of your thigh. Because they don’t touch your kneecap, there is no anterior pain nor risk of a fracture.
However, you can feel:
- less strength in your hamstring, that is when flexing your knee
- sometimes, the graft is not as “tight” as it should be, it loosens up a bit
· Quadriceps tendon
Your quadriceps tendon is at the end of your thigh, on the front, and it attaches to the kneecap, too.
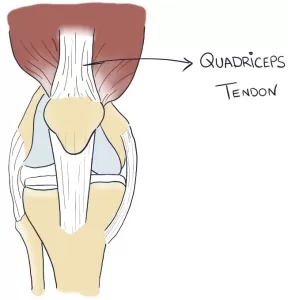
Because it’s the largest tendon, it can be a good fit for large patients (because they need large grafts).
Also, it’s a good option to treat failed ACL reconstructions. In that case, you don’t want to use a patellar tendon again—you’ll weaken it too much. Instead, you can go for the large strong quadriceps tendon.
Because this tendon attaches to the kneecap, too, it can also cause anterior pain and kneecap fractures. Other drawbacks are:
- it may loosen
- the scar is quite large, and in front of your knee and thigh
Using allografts for ACL reconstruction
As we said, allografts come from donors. One good thing about them is surgery time will be lower, because they won’t have to harvest the graft from you. Surgery will be just placing it in your knee.
Also, for the same reason, your scars will be less and smaller.
As for their safety, every donor undergoes strict tests to rule out they have some transmittable disease such as HIV or hepatitis. So it’s very safe.
There is only one disadvantage. Some doctors say allografts may not be 100% as effective as autografts. However, they haven’t proven this, it’s just their perception.
Apparently, there may be slightly higher rates of failure in professional athletes, so we usually choose autografts instead for young active athletes.
Leave a Reply